Other Treatment Methods
.webp)
Cataract
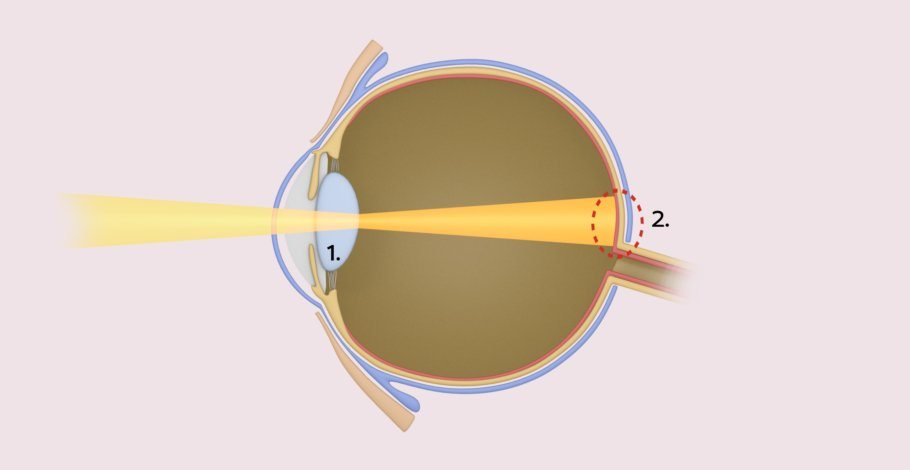
Cataracts are not a disease in the true sense, but rather the result of the natural aging of the human lens. This gradually becomes cloudy, so that the previously crystal-clear lens appears white-gray. Over time, the clouding leads to reduced light transmittance. As a result, patients see less well in everyday life, for example when driving or reading. Even a new pair of glasses cannot improve this condition. Surgery can be advisable if patients increasingly feel restricted due to reduced visual performance.
Before cataract surgery
First, the eye is thoroughly examined and measured to achieve an optimal surgical outcome. Based on the findings, the ophthalmologist chooses a suitable artificial lens together with the patient, which will replace the clouded lens. Nowadays, very individualized solutions are possible, such as lenses that can also correct more complex vision defects and often even make glasses superfluous.
Intraocular lenses (IOL)
Choosing the right lens model is essential for a perfect result. There are three different types of lenses: monofocal, toric, and multifocal lenses. All modern premium lenses have an integrated UV protection that absorbs 100 percent of harmful UV light.
Monofocal lenses
This lens, just like the human lens in old age, provides only one focal point. It is used to correct Short- or farsightedness. Typically, the artificial lens is chosen so that the focal point is in the distance. As a result, patients need reading glasses for near vision. If there are more complex vision errors like severe astigmatism (astigmatism) present, these lenses are not sufficient to completely correct the vision error.
Toric lenses
These lenses correct not only nearsightedness or farsightedness but also astigmatism. They are individually manufactured for each patient and implanted according to the individual astigmatism. The LED corneal topographer Cassini opens up a new dimension by measuring astigmatism with unprecedented precision. Its results are directly fed into the Lensar® Laser, which identifies and marks the true axis of astigmatism using integrated iris recognition. Thus, the surgeon can align the lens much more precisely than with conventional manual marking.
Multifocal lenses and new macula specialty lens
TRIFOCAL
Unlike monofocal lenses, these lenses offer the possibility of being able to dispense with glasses after the operation. The trifocal lenses have several focal points: objects at close range (newspaper), at medium distance (computer, speedometer), and at a distance (theater, opera). During the day this works very well, but at night, bright light sources like LED lamps or the red taillights of cars produce very annoying circular or star-shaped halos (called halos or glare), which significantly impair driving at night.
EDOF
The abbreviation stands for Extended Depth Of Focus. EDOF lenses were developed to minimize the above-mentioned disturbing side effects of trifocal lenses. This is not achieved by all manufacturers, but the EDOF segment lenses (e.g. Acunex vario) do not exhibit these disturbing light effects. However, very small printed texts (package inserts for medicines, stock quotes in newspapers, or the well-known small print in contracts) can only be deciphered with slight reading glasses. An alternative concept, such as the blended vision according to the Düsseldorf scheme, developed by the premium doctors there, can compensate for this small disadvantage.
MONOVISION – BLENDED VISION
An old but still well-known system to dispense with glasses in everyday life. It is based on the principle that we have a dominant and a non-dominant eye. (Similar to our hands: right-handed or left-handed.) The dominant eye is corrected for distance and the non-dominant eye for near vision. After an adaptation period of 3 to 12 months, this system also works very well, especially without disturbing glare at night. It is a good alternative treatment when neither trifocal nor EDOF lenses are recommended due to anatomical peculiarities.
EXTENDED MACULAR LENS
This lens was specifically designed for patients with macular diseases designed because too often after a cataract surgery with an existing macular disease (AMD), patients had worse vision than before the procedure. The Eyemax Mono lens supports the brain’s ability to use the healthiest areas of the macula to achieve the best possible result. Combined with glasses, this lens system can also magnify the image. In a way, it is both simple and complex at the same time! Optimizing the image across the entire macula is a revolutionary way to help patients whose eye condition affects central vision – such as in AMD or macular edema.
cataract surgery procedure
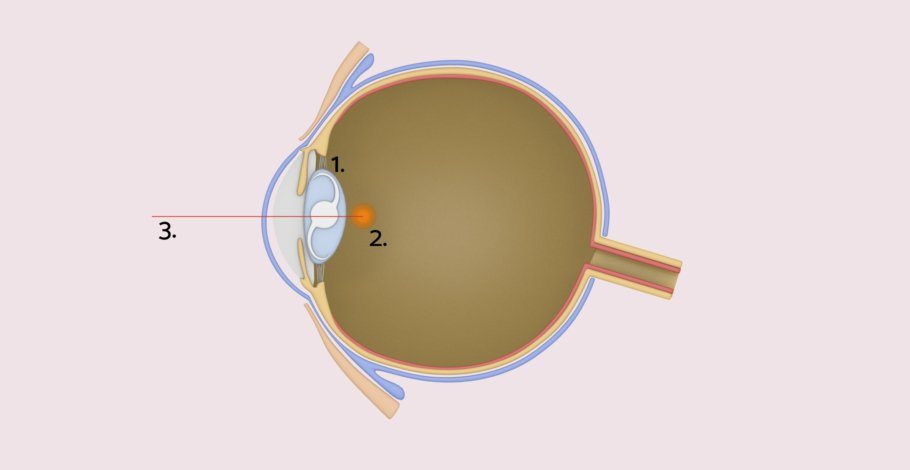
The surgery is performed on an outpatient basis under local anesthesia, often with light sedation (twilight sleep). The procedure takes 10 to 20 minutes. If both eyes need to be treated, the second eye is operated on a few days or much later. Cataract surgery can be performed manually as well as with the femtosecond laser. According to the latest scientific findings, the laser is more precise, safer, and gentler than the human hand. The laser even corrects astigmatism with the highest accuracy.
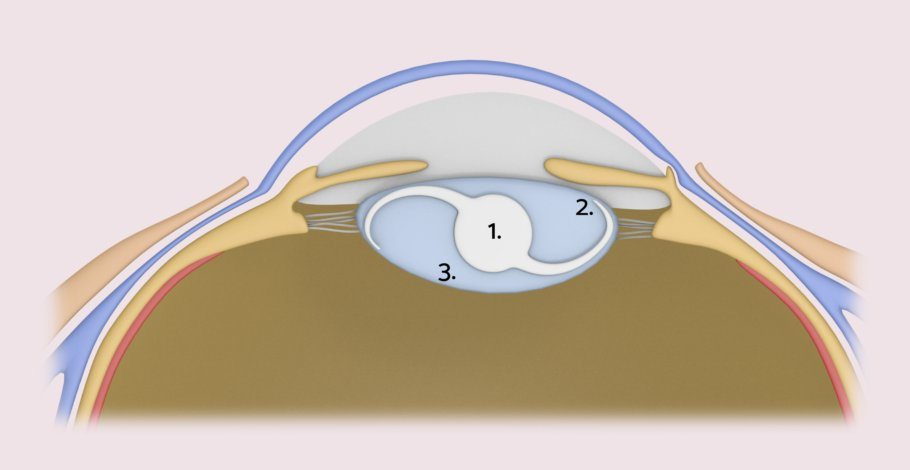
In the laser cataract surgery, the laser makes an approximately 2-millimeter fine incision at the edge of the cornea to the lens and also fragments the cloudy, natural lens of the eye. The eye surgeon then removes the lens from the capsule bag (the support apparatus for the human lens). The capsule bag also serves as a suspension for the new artificial lens.
cataract surgery with the femtosecond laser
Thanks to femtosecond laser technology, individual steps of traditional cataract surgery can now be automated and performed very gently. The opening of the human lens capsule, the dissection and loosening of the cloudy lens core as well as the incision at the edge of the cornea are carried out by the laser in just a few seconds. Apart from the far greater precision of the laser compared to the human hand, the surgery becomes gentler and safer. This is confirmed by all current scientific publications.
risks of cataract surgery
Cataract surgeries are among the most common and safest operations worldwide. Complications such as infections in the eye occur very rarely and can be well treated. However, sometimes the refractive power of the implanted artificial lens may not be one hundred percent accurate. Therefore, patients must be informed before the procedure that even a modern artificial lens does not have the capabilities of a youthful, human lens.
After the cataract surgery
After the surgery, the ophthalmologist applies a sterile dressing, which is removed during the postoperative check-up the next day. In the first days and weeks after the surgery, the eye may tear up more frequently and be reddened. Visual acuity and the refractive power of the eye may fluctuate in the first four to six weeks but should steadily improve. If necessary, eyeglasses will be adjusted no sooner than six weeks post-operation. Patients can return to work after just a few days to a week. For a speedy recovery, they should avoid sports, swimming, and other physical exertions for the first six weeks, and refrain from rubbing or applying pressure to the operated eye.
Experts for this Treatment Method

- Modern Ophthalmology
Dr. Mirka R. Höltzermann
Augenpraxis Dr. Höltzermann, Dr. von Schnakenburg, Augenpraxis Dres. Höltzermann & von Schnakenburg
- Modern Ophthalmology
Dr. med. Ilya Kotomin
Smile Eyes Leipzig
- Modern Ophthalmology
Priv.-Doz. Dr. med. Daniel Pilger
Smile Eyes Berlin
- Modern Ophthalmology
Raphael Neuhann (FEBO)
Opthalmologikum Dr. Neuhann / Augentagesklinik am Marienplatz
- Modern Ophthalmology
Dr. med. Tabitha Neuhann
Opthalmologikum Dr. Neuhann / Augentagesklinik am Marienplatz
- Modern Ophthalmology
Prof. Dr. med. Tanja M. Radsilber
Augenzentrum Prof. Dr. med. Holzer & Prof. Dr. med. RabsilberAll Experts in this Department
Show All
- Modern Ophthalmology
Dr. Christine Heun
IRISIOvital Praxis für Augengesundheit- Modern Ophthalmology
Dr. Mirka R. Höltzermann
Augenpraxis Dr. Höltzermann, Dr. von Schnakenburg, Augenpraxis Dres. Höltzermann & von Schnakenburg- Modern Ophthalmology
Dr. med. Ilya Kotomin
Smile Eyes Leipzig- Modern Ophthalmology
Priv.-Doz. Dr. med. Daniel Pilger
Smile Eyes Berlin- Modern Ophthalmology
Raphael Neuhann (FEBO)
Opthalmologikum Dr. Neuhann / Augentagesklinik am Marienplatz- Modern Ophthalmology