Why Standard Values Are Not Enough
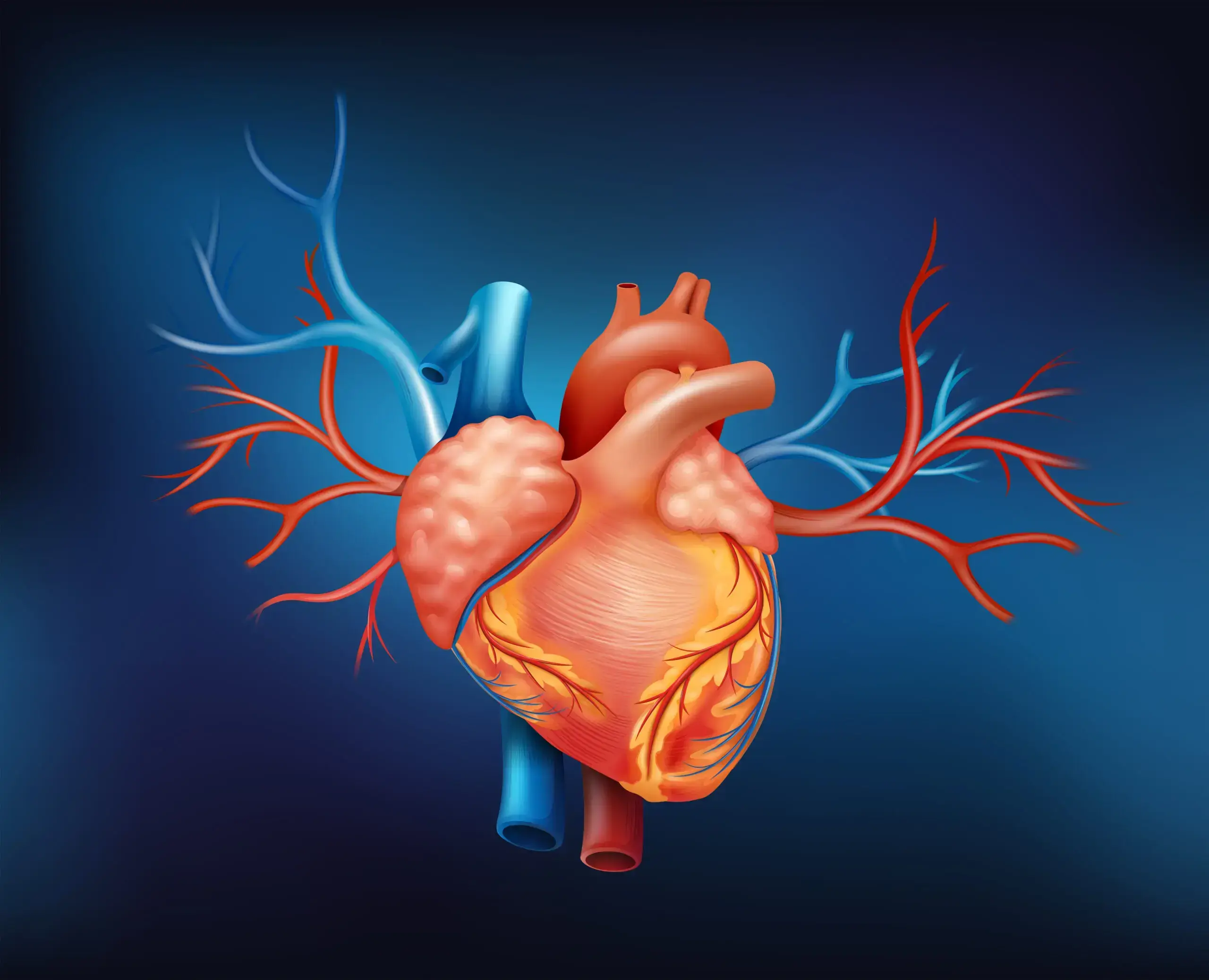
Legal preventive care focuses on blood pressure and total cholesterol, with men over 65 also getting an aortic screening. But this falls short. Total cholesterol, for example, doesn't indicate how many risky particles are circulating in the blood, promoting deposits in vessels, known as atherogenic particles. And even ultrasound examinations of large vessels only show changes once the disease is advanced. Particularly critical: The coronary arteries, which are the most vulnerable and where the risk is highest, remain invisible in this routine.
This inadequate diagnostics not only affects members of the statutory health insurance. Many private health insurances now also align their coverage with the guidelines of statutory preventive care. As a result, essential preventive diagnostics are often not covered there either. Instead of enabling progress, prevention is based on outdated standards.
Speaking of outdated:
Cholesterol in Context
Cholesterol is not an enemy but a vital building block. It stabilizes cell membranes and serves as a precursor for vitamin D, bile acids, and hormones like cortisol, testosterone, or estradiol. About 80 percent is produced by the liver itself; only a small part comes from diet. Therefore, the risk is determined not by the sheer amount, but by the transport form and the combination with genetic, metabolic, and inflammatory factors.
A Multidimensional Risk Diagnostics
Modern prevention must consider many levels, including biomarkers that are now readily available.
Vascular mechanics
Permanently elevated blood pressure acts like constant waves on the delicate inner lining of the vessels, the endothelium. Tiny injuries occur, platelets settle, fats accumulate. This creates the basis for dangerous plaques.
Lipidology
This is about the transport forms of cholesterol and fats in the blood:
ApoB is the central marker for the number of atherogenic particles. The more particles, the greater the risk of deposits.
Complete lipid paneli.e. LDL, HDL and Triglyceride including subfractionation of lipids into particle number, size, and density.
Lipoprotein(a), or Lp(a) for short, is a special form of LDL cholesterol to which an additional protein is attached. This not only promotes deposits but also inflammation and blood clots. Guidelines recommend a one-time measurement of Lp(a) in all adults. For women, it is advisable to check the value additionally before and after menopause, as the cardiovascular risk increases significantly during this phase of life. It is a strong genetic risk factor.